This is an online E log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent. Here we discuss our individual patient's problems through series of inputs from global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs. This E log book also reflects my patient-centred online learning portfolio and your valuable inputs on the comment box is welcome."I've been given this case to solve in an attempt to understand the topic of "patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with a diagnosis and treatment plan
65 yr old male resident of nalgonda weaver by occupation came to OPD with
Chief complaints
Swelling in the right lower limb and scortum since 5 days
Multiple blisters on the leg since 5 days
Fever since 5 days
History of presenting illness
He was apparently asymptomatic 5 days ago then he developed swelling in right lower limb upto thigh (gradually progressive from foot to thigh)along with scortum which is associated with pain - sudden in onset , gradually progressive , pricking type, aggravated on walking , releived on rest
Multiple blisters on right leg, associated with local rise of temperature, moderate fever(102°f),skin changes, pigmentation
Not associated with burning micturation, urinary incontinence
Past history
Known case of filariasis since 15 yrs and on medication ( Diethylcarbamazine)
Not a k/c/o HTN,DM , epilepsy,TB,CAD,CVD,asthma
Personal history
Diet :mixed
Appetite : decreased
Sleep: adequate
Bladder and bowel movements : normal and regular
Addictions : consumes alcohol occasionally
No allergies
Treatment history
Diethylcarbamazine since 15yrs (takes medicine only after noticable swelling)
Chymoral forte -takes when there is pain
Family history
Non significant
General examination
Patient is conscious,coherent and cooperative
Well oriented to time place and person
Moderately built and nourished
No pallor,icterus, cynosis, clubbing, koilonychia,
Lymphadenopathy:enlarged inguinal and popliteal lymph nodes
Pedal oedema -pitting type ,from foot upto thigh
Vitals
Bp:100/60 mm hg
Temp:98
RR:21cpm
PR:78bpm
Systemic examination
CVS:S1,S2 heard ,no murmurs
CNS: no focal neurological deficit
Resp: Bilateral air entry present,normal vesicular breath sounds heard
Per abdomen: soft and non tender
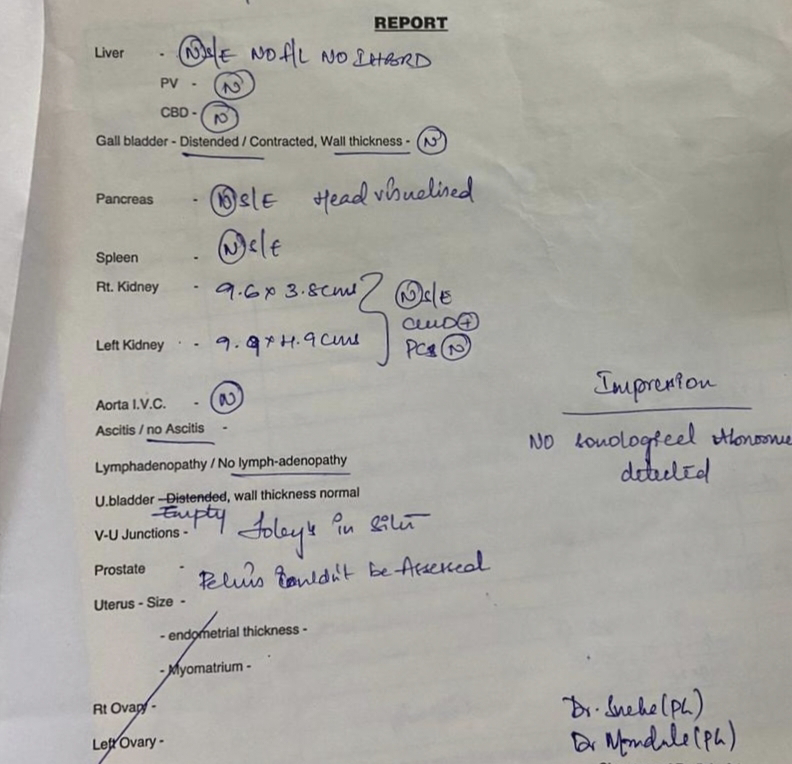
Investigations
Treatment history
1)IV fluids (normal saline 75ml/hr)
2) Inj.PAN 40 mg OD
3)Tab.Dolo 650 mg
4) Inj. NEOLOL 1gm
5) Inj.PIPTAZ 4.5gm



















Comments
Post a Comment