Pulaparthi Jahnavi
GENERAL MEDICINE BIMONTHLY ASSESSMENT-AUGUST 2021
Pulaparthi Jahnavi
3rd Sem
QUESTION 1:
Please go through the long and short cases in the first link shared above and provide your critical appraisal of the captured data in terms of completeness, correctness and ability to provide useful leads to analyze the diagnostic and therapeutic uncertainties around the cases shared.
https://2018-21batchpgy3gmpracticals.blogspot.com/2021/08/18100006003-case-presentations.html?m=1
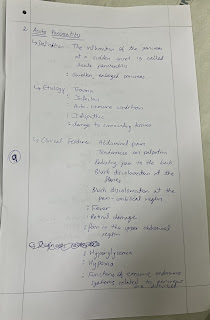
LONG CASE:
A case of acute glomerulonephritis , due to sec. amyloidosis due to chronic poorly treated seronegative erosive rheumatoid arthritis .
Completeness :
The E-log was complete in all factors . It included chief complaints , present history , past history , medical/surgical history , personal history , family history , social & educational history , immunization history .
This elog had everything one could have asked for ; for a better understanding of the case and to treat in a better way .
Review on the case :
The case was beautifully presented in detail , which is almost closely knit with his details , which seemed like a story to me , like a step-to-step detailed explanation .
Evolution of symptomatology was described in a detail manner .
There was also a detailed explanation of the patient's acute and chronic problem .
General examination was done in a much detailed way ; in different positions with clear documentation .
Clinical images of the patient and investigations were added with deidentification .
Systemic examination with detailed inspection , palpation , range of movements was explained .
Diagnostic approach and treatment was also well explained .
Correctness :
All the data provided in the E-log is correct .
SHORT CASE 1:
Idiopathic Parkinson's disease stage 1 with denovo HTN & multiple system atrophy - parkinsonian type ( MSA-P )
Completeness :
The elog was complete . it included chief complaints , history of presenting illness , history of past illness , medical / surgical history , personal history , family history , social & education history , immunization history.
Review on the case:
The case was beautifully presented in detail , which is almost closely knit with his details , which seemed like a story to me , like a step-to-step detailed explanation .
Evolution of symptomatology was described in a detail manner
CNS examination was described extremely well with all detailed documentation of reflexes etc.
Clinical images of the patient and investigations were added with deidentification .
Correctness :
All the data pirovided in the E-log is correct .
SHORT CASE 2:
Iatrogenic cushings syndrome secondary to topical clobetasol application all over the body for approx. 1 yr.
Completeness :
this elog was little incomplete acc. to me as it didn't include his past history , family history , treatment history , personal history.
Review on the case:
Evolution of current symptomatology was described beautifully .
De-identified clinical images in the presentation , showed us the condition of the pt. clearly .
His follow up details were also neatly documented .
Correctness :
All the data provided in the E-log is correct .
QUESTION 2:
Please analyze the above linked long and short cases patient data by first preparing a problem list for each patient in order of perceived priority (based on the shared data) and then discuss the diagnostic and therapeutic uncertainty around solving those problems.
LONG CASE-
PROBLEM LIST:
Generalized edema.
Facial puffiness with pedal edema.
Pitting type pedal edema, extending upto the middle of his legs.
Breathlessness, palpitations or chest pain.
Decreasing urine output
Debilitating early morning pains and limitation of movements in his hands, wrists and feet, which usually lasts for about an hour
Burning sensation in his eyes
Proteinuria causing anasarca likely due to glomerular pathology.
DIAGNOSIS-
Bilaterally Symmetric Chronic Progressive Inflammatory Peripheral Polyarthritis Acute Glomerulopathy (Glomerulonephritis / Nephrotic syndrome)
Secondary Amyloidosis
Dilutional Hyponatremia secondary to Anasarca due to Glomerulonephritis
Hyperuricemia likely due to decreased Uric Acid Excretion Precipitating Gouty Arthritis
Anemia of Chronic Disease secondary to Poorly Treated Rheumatoid Arthritis.
TREATMENT PLAN-
Tab. PREDNISOLONE P/O 20 mg OD
Tab FEBUXOSTAT P/O 80 mg OD
Haemodialysis for worsening renal dysfunction
SHORT CASE 1-
PROBLEM LIST:
progressive asymmetric involuntary movements of his right index and middle fingers.
stiffness in his wrists (Right>Left), which has now ascended to his elbows
difficulty in taking the stairs
hasn't been having morning erections since 2 months
reports a loss of sexual desire.
He also says that since 2 months his bowel habits have been incredibly erratic, in that he sometimes has an immediate urge to defecate and sometimes goes 2 to 3 days with constipation.
has been speaking in a monotonous drab since 2 months
DIAGNOSIS-
1. Idiopathic Parkinson's Disease Stage 1 with denovo HTN.
2. Multiple System Atrophy - Parkinsonian Type (MSA-P).
TREATMENT PLAN-
1. Tab. Syndopa Plus 125 mg QID
2. Tab. Syndopa 125 mg CR OD
3. Tab. Telma 40 mg OD
SHORT CASE 2:
PROBLEM LIST:
-Itchy Ring leisons over arms ,abdomen ,thigh and groin since 1 and half year .
-Purple stretch marks all over abdomen ,lower back ,upper limbs ,thighs since 1 year .
-Abdominal distension and facial puffiness since 6 months.
- Pedal edema since 3 months.
- Low back ache since 3 months .
- Feeling low , not feeling to talk to anyone.
- Weight gain and decreased libido since 3months.
- Loss of libido and erectile dysfunction since 2 months .
-Multiple hyperpigmented plaques over lower limbs and abdomen
-Easy fatigue, weakness and lower backache
-Moon face present, thick skin
-poor healing over leg ulcers
-Acne present over face
-Acanthosis nigrans noted over neck
-GYNECOMASTIA PRESENT
-Buffalo hump present
-Sparse scalp hair
-Difficulty in getting up from chair
DIAGNOSIS :
-IATROGENIC CUSHINGS SYNDROME SECONDARY TO TOPICAL CLOBETASOL APPLICATION ALL OVER BODY FOR APPROXIMATELY ONE YEAR.
-TINEA CORPORIS
-DENOVO HTN .
TREATMENT PLAN :
Ointment AMLORFINE
FUSIDIC ACID CREAM.
SALINE COMPRESS OVER LEISONS
Tab.Telma 20 mg od .Due to low cortisol level
pt was started on TAB HIZONE 15 mg per day in three divided doses @ 8am ,12 pm and 4 pm.
0.4 ML OF ACTOM PROLONGATUM INJECTION (ACTH) INTRA MUSCULAR @ 7am
Tab Shelcal 500 OD and Tab Vit D 3 Od.
Tab ULTRACET /PO/SOS.
Tab Itraconazole 100 mg bd. And lulifin cream and tab levocitrixine 5mg od.
QUESTION 3-
Testing competency in "Evidence based medicine": Include the review of literature around sensitivity and specificity of the diagnostic interventions mentioned and same around efficacy of the therapeutic interventions mentioned for each patient.
LONG CASE :
Investigations done are:-
Current Admission - Blood tests
Blood work from previous presentations to hospital. RA factor was negative
24hrs urinary protein: 1500 mg
24hrs urinary creatinine: 0.8
Urine Microscopy - Freshly voided urine sample was centrifuged at high speed (> 2700 RPM) and sediment collected and fixed on glass slide and examined under microscope at 400 (10x * 40x) showed DYSMORPHIC RBCs (black circles) and occasional pus cells (red circles). Dysmorphic RBCs were those that had altered shape, microcytic or with membrane defects.
Efficacy of Treatment given:-
Tab. PREDNISOLONE P/O 20 mg OD:-It is used to treat conditions such as arthritis, blood problems, immune system disorders, skin and eye conditions, breathing problems, cancer, and severe allergies. It decreases your immune system's response to various diseases to reduce symptoms such as pain, swelling and allergic-type reactions.
Tab FEBUXOSTAT P/O 80 mg OD:-class of medications called xanthine oxidase inhibitors. It works by decreasing the amount of uric acid that is made in the body. Febuxostat is used to prevent gout attacks but not to treat them once they occur.
Haemodialysis for worsening renal dysfunction
SHORT CASE 1:
Investigations done are:-
-ECG: Shows Sinus Tachycardia with pseudo infarct pattern in leads I and aVL with dagger q waves in the same leads,No late intrinsicoid deflection of R wave with modified Cornell criteria showing LVH.
-2 D Echo : Grade II diastolic dysfunction
Efficacy of Treatment given:-
-Tab. Syndopa Plus 125 mg QID: is a combination of two medicines used to treat Parkinson's disease. It is one of the most effective medications to relives symptoms of Parkinson's disease such as tremor, muscle stiffness and difficulty moving.
-Tab. Syndopa 125 mg CR OD: is a combination of two medicines which are Levodopa and Carbidopa. This medication is used to treat the symptoms of Parkinson's disease like tremors , stiffness and slowness of movement.
-Tab. Telma 40 mg OD: is a medicine used to treat high blood pressure and heart failure. Lowering blood pressure helps to prevent future heart attack and stroke.
SHORT CASE 2:
Investigations done are:-
CBP - HB - 13.4 g/dl
TLC - 6,800
PLT - 1.5 lakhs.
RBS - 139 mg/dl
CUE - ALBUMIN - +1
SUGARS - NIL .
PUS CELLS - 3-4
RBC - NIL .
LFT - TB -1.03
DB-0.21
ALBUMIN - 3.9
RFT - UREA - 22
SERUM CREATININE -0.6
ELECTROLYTES - NA - 136
K- 4
CL-98
USG ABDOMEN - NORMAL.
ECG - SINUS TACHYCARDIA
LVH PRESENT.
Efficacy of Treatment given:-
-Tab.Telma 20 mg od: due to low cortisol level
-TAB HIZONE 15 mg: is prescribed for Severe allergic reactions,allergic conditions,Cancer,Skin disorders,Eye disorders.
-Tab Shelcal 500 OD and Tab Vit D 3 Od: To treat vitamin D and Calcium deficiency.
-Tab ULTRACET /PO/SOS: is a combination of two medicines that are used for short term relief of pain, inflammation, and swelling in conditions that affect joints and muscles.
-Tab Itraconazole 100 mg bd: to treat a variety of fungal infections.
-Tab levocitrixine 5mg od: relieve runny nose, sneezing, redness, itching.
QUESTION 4:
Testing competency in patient data capture and representation through ethical case reporting/case presentation with informed consent :
Share the link to your own case report this month of a patient that you connected with and engaged while capturing his her sequential life events before and after the illness and clinical and investigational images along with your discussion of that cases.
(Haven’t got a chance to make a elog)
QUESTION 5:
Testing scholarship competency in
logging reflective observations on your concrete experiences of this last month :
This telemedical learning and Elogging experience was Good, But most important thing we are missing was direct exposure to clinical postings.
Hope to attend clinicals directly in the hospital very soon.
Going through elogs that are made by my seniors provided a widespread exposure to variety of cases in a short span of time.
While going through all the blogs that are prepared by my seniors I learnt a lot and it will be useful for me in future for sure.
We are learning how to approach a patient,about History taking and also how to present the case.
Overall It is a great experience,gave scope for interacting and we are learning a lot from this postings.

Comments
Post a Comment